All published articles of this journal are available on ScienceDirect.

Multiply Recurrent Calcaneal Osteochondroma: A Case Report
Abstract
Introduction/Background
Osteochondromas are the most common benign bone tumors, typically presenting as cartilage-capped bony projections on the external surface of bones. Recurrent isolated osteochondromas are uncommon and have a low recurrence rate after surgical resection. Previous literature has documented solitary osteochondromas in the calcaneus, but to our knowledge, recurrent cases have not been reported.
Case Presentation
A 20-year-old female presents after the removal of a calcaneal osteochondroma by podiatry at the age of 12 and again at the age of 17. The lesion recurred again at age 18, and the patient was then referred to orthopedic oncology. The patient’s primary presenting symptom was a slowly enlarging bump on her heel. The lesion was again excised, and the pathology was consistent with osteochondroma. She had no recurrence until 23 months postoperatively. At that point, she presented again with a bump slowly increasing in size as well as pain after several months of significantly increased walking while abroad. The lesion was again removed with care taken to remove all satellite lesions and to bur the main lesion down to normal calcaneus. The patient has had no recurrence at the most recent follow-up of 6 months.
Conclusion
This case report highlights the unusual presentation of a multiply recurrent calcaneal osteochondroma, emphasizing the need for comprehensive surgical excision and diligent follow-up. Incomplete resection is the most common reason for recurrence. However, given the lesion's location, this case raises the question of whether repetitive stress from increased walking may have contributed to its recurrence.
1. INTRODUCTION
Osteochondromas are the most common benign bone tumors, accounting for 20-50% of benign bone tumors and 9% of all bone tumors. The exact incidence of osteochondromas is unknown since many are asymptomatic and remain undiagnosed. When lesions are found, they are typically seen within the first four decades of life, with 75% occurring before age 20. They are typically discovered incidentally on radiographs obtained for other reasons. The second most frequent presentation is a painless palpable lump on the involved bone [1]. Osteochondromas typically present as cartilage-capped bony projections on the external surface of bones. These lesions can be either sessile or pedunculated and are most frequently found in the metaphyseal region of long bones. Approximately 85% of osteochondromas occur as solitary lesions, while the remaining 15% are associated with Hereditary Multiple Osteochondromas (HMO), a disorder characterized by multiple osteochondromas [2]. HMO results from a mutation in either the EXT1 or EXT2 genes responsible for the EXT1 and EXT2 proteins. These proteins are implicated in several growth signaling pathways in the normal epiphyseal growth plate [2]. Osteochondromas have a predilection for long bones, with almost half being located around the knee (30% in the distal femur, 15-20% in the proximal tibia). Osteochondromas in the feet and hands account for approximately 10% of cases [1]. As most are asymptomatic, the overall societal burden of osteochondromas is low, with the most concerning feature being the rare potential for malignant transformation into a chondrosarcoma (1-2% of cases) [2]. When symptomatic and especially when malignant transformation is a concern, surgical resection is the mainstay of treatment [1, 2].
The calcaneus is a relatively rare location for osteochondroma formation [3-5]. Patients with calcaneal osteochondromas typically present with localized pain, swelling, and sometimes mechanical symptoms such as gait disturbances. In rare cases, complications like tarsal tunnel syndrome can occur due to nerve compression [3]. The lesion is often discovered incidentally or due to symptoms arising from its size or location [4, 5]. However, they can cause symptoms due to mechanical irritation, compression of adjacent structures, or complications such as fractures, vascular or neurologic compromise, and malignant transformation.
Radiographically, osteochondromas are identified by the continuity of the cortex and medullary bone with the host bone. Surgical excision is the primary treatment for symptomatic osteochondromas. Complete resection, including the cartilage cap and perichondrium, is essential to minimize recurrence [6]. In cases of recurrent lesions, thorough surgical excision remains the mainstay of treatment [2].
This case report highlights a unique presentation of an osteochondroma, detailing the clinical, radiological, and pathological findings, as well as the therapeutic approach and outcomes. While other cases of calcaneal osteochondroma have been reported, to our knowledge, this is the first case of a calcaneal osteochondroma with multiple recurrences.
2. CASE PRESENTATION
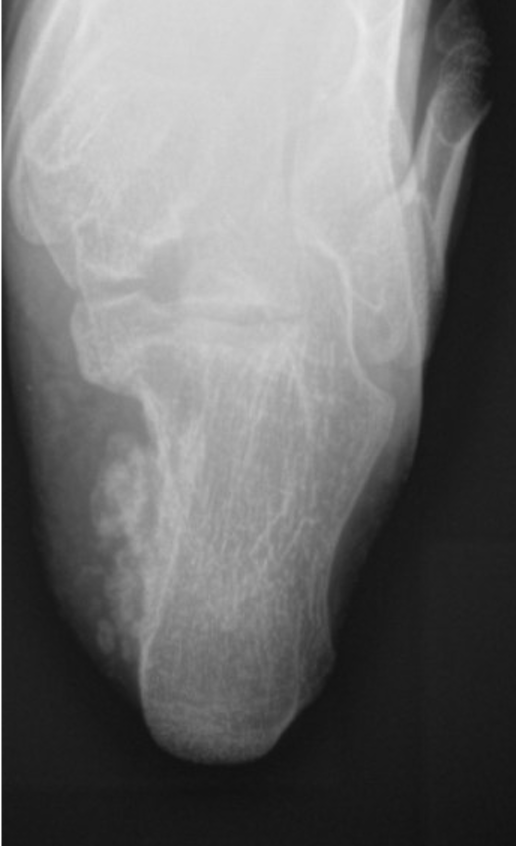
This is a 20-year-old female who presented with a history of a multiply recurrent osteochondroma of her left calcaneus removed in the past by Podiatry. The first excision was when she was 12 years old, and the lesion was thought to be an accessory calcaneus. She was found to have a recurrence at the age of 17, and the lesion was again removed by podiatry. Pathology from this case was consistent with an osteochondroma. It was then, at age 18, that the patient presented to orthopedic oncology for recurrence of the lesion. She presented with a painful bump on her heel that had been slowly increasing in size, similar to her previous presentations to podiatry. Axial radiograph and a select cut of the MRI taken at the time of her initial evaluation by orthopedic oncology are shown in Figs. (1 and 2). Given that the patient was symptomatic, the decision was made to proceed with surgical resection.

Axial radiograph demonstrating bony outgrowth off the posterior aspect of the calcaneus, findings consistent with osteochondroma.
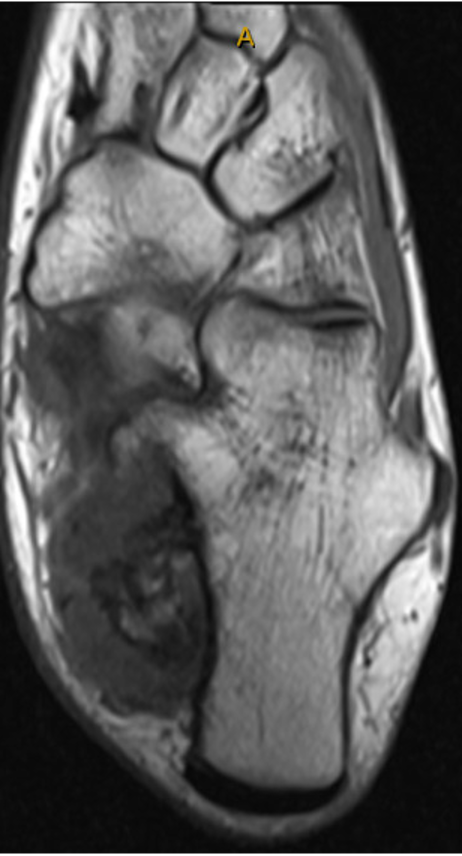
Selected axial cut from MRI imaging demonstrating bony outgrowth from the posterior medial aspect of the calcaneus consistent with osteochondroma; there is a cartilage cap ~15mm, and the medullary contents of the outgrowth appear in continuity with the calcaneus.
The patient was taken to the operating room for lesion excision, marking the patient’s third excision and the first performed by an orthopedic oncologic surgeon. An L-shaped incision was utilized, extending from proximal to the medial malleolus just anterior to the Achilles tendon and then gently curving to incorporate the previous longitudinal incision along the medial aspect of her plantar foot. The tarsal tunnel was opened using tenotomy scissors, and the posterior tibial artery and vein as well as the tibial nerve, were identified. These were adhered to the mass, and meticulous dissection of the adhesions of the neurovascular structures from the mass was required. Once the neurovascular structures were released from the mass and protected, a previously applied tourniquet was inflated, improving visualization of the mass. It appeared lobulated and cartilaginous, arising from the medial border of the calcaneus. It was fixed and immobile. Fluoroscopy was used to identify the normal cortex, and curved osteotomes were used to osteotomize the medial cortex of the calcaneus to release the tumor and restore the calcaneus to a normal contour. Upon doing this, it was evident that the tumor had a cancellous base in continuity with the calcaneus, consistent with an osteochondroma. Given its large size and the mass’s proximity to adjacent structures, it was necessary to remove it in a piecemeal fashion. Care was taken to ensure no cartilaginous fragments were left within the soft tissues. Final fluoroscopy demonstrated no definite evidence of residual tumor. A bur was used to burr the bone at the tumor bed to normal-appearing cancellous bone. The bone was cauterized at the site, and bone wax was applied. The tourniquet was then released, the incision was closed in layers, and the patient was taken to the post-anesthesia care unit. Fragments sent to pathology confirmed the mass as an osteochondroma. She did well postoperatively but subsequently developed recurrence of the lesion at her two-year follow-up visit.
Her recurrence occurred after studying abroad, when she was walking more. This recurrence marked the fourth presentation of the lesion. She initially noticed a bump on her shoe, which grew in size over the next few months and became increasingly painful. The recurrence showed signs of both a recurrent primary mass confluent with the calcaneus and satellite lesions within the soft tissues, as seen on the radiograph in Fig. (3). Given the multiple recurrences, the possibilities of an atypical cartilaginous tumor or even low-grade chondrosarcoma were discussed. Her previous imaging studies and histologic specimens were re-evaluated at a multidisciplinary tumor board composed of multiple orthopedic oncologic surgeons, radiologists, and pathologists, who confirmed that they appeared most consistent with benign osteochondromas.
Axial radiograph obtained at 23 months follow-up with evidence of local recurrence.
As she was having progressive pain and difficulty with shoe wear, the decision was made to proceed with an attempt at repeat excision. The patient was again taken to the operating room, marking the fourth excision of the mass. After induction of general anesthesia, a tourniquet was applied and inflated. The same incision was utilized. Several satellite lesions were present in the soft tissues, distinct from the primary lesion. These were dissected and removed, each as a single piece. The primary mass wrapped around the medial calcaneus, which prevented en bloc resection; therefore, a series of osteotomies was performed to break the mass into several large fragments, which were then removed until a normal-appearing calcaneus was visible. After removal of the larger fragments, a rongeur and osteotomes were used to ensure no further cartilage was evident along the medial calcaneus. The tumor bed was carefully inspected, and no additional cartilage fragments were found. The wound was copiously irrigated, and the tourniquet deflated. Bone wax was applied to the tumor bed. The wound was closed in a layered fashion. The patient was transferred from the operating room to the post-anesthesia care unit without complication. The specimen was sent for pathology, which again confirmed benign osteochondroma. She did well postoperatively. She was made non-weight-bearing in a CAM boot to protect the incision and to avoid microtrauma to the osteochondroma site for 8 weeks, at which time she was transitioned to progressive weight-bearing as tolerated in regular shoes. Radiographs taken at her 6-month postoperative visit showed no evidence of recurrence, as shown in Figure 4.

Axial radiograph obtained at 6 months of revision surgery demonstrating no recurrence.
3. DISCUSSION
The case of a multiply recurrent calcaneal osteochondroma is particularly noteworthy due to its rarity. Previous literature has documented solitary osteochondromas of the calcaneus, including two cases of lesions removed that subsequently recurred. There are also documented cases of recurrent osteochondromas in the finger, proximal humerus, distal tibia, and mandible. However, to our knowledge, multiply recurrent cases in the calcaneus have not been reported [4, 5, 7-13]. This case underscores the importance of thorough surgical excision with clear margins to minimize the risk of recurrence, as incomplete resection is a known risk factor for local recurrence [1, 5]. While en bloc resection of the tumor in this patient’s case would have been preferred to ensure complete removal of the lesion, the surrounding neurovascular structures, as well as the size of the tumor, prevented this. Therefore, the decision was made to remove the tumor in pieces in both cases. The lesion was resected in this fashion until normal-appearing calcaneal bone was visualized in both cases, using a rongeur, bur, or osteotomes, and no visible lesion remained, ensuring, as much as possible, a thorough resection.
The clinical presentation of calcaneal osteochondromas can vary. Symptoms may include localized pain, swelling, and mechanical issues such as gait disturbances [3, 4]. In this case, the recurrent nature of the tumor suggests a need for vigilant postoperative monitoring and possibly more aggressive surgical management at index surgery. Imaging modalities such as X-ray and MRI are crucial for diagnosis and follow-up, particularly to assess for signs of malignant transformation, which, although rare, can occur [1, 6, 7]. Garrison et al. reported that among 75 cases of chondrosarcomas secondary to osteochondromas seen at the Mayo Clinic, only one case involved the calcaneus, and this was in a patient with hereditary multiple osteochondromas [14].
The recurrence rate of isolated osteochondromas after surgical resection is generally low, with studies reporting rates of less than 2% when complete resection is achieved [1]. The management of recurrent osteochondromas remains largely the same as that of a primary osteochondroma, involving surgical resection with the goal of complete removal to prevent further recurrence. Histological examination is essential to rule out malignancy, especially in recurrent growths [1, 7]. Given the rarity of calcaneal osteochondromas, this case contributes insight into their clinical behavior and management strategies.
This patient’s lesion bears some resemblance to a parosteal osteochondromatous proliferation, also known as Nora's lesion. There are, however, distinct differences. With an osteochondroma, the bony outgrowth is continuous with the underlying medullary cavity, whereas in Nora’s lesion, the lesion originates from the periosteum and is attached to the outer cortex. Histologically, there were no characteristics supportive of Nora’s lesion. Specifically, there was no evidence of a disorganized mix of bone, cartilage, and fibrous tissue. Fibrous components were absent, and intertrabecular spaces lacked spindle-cell proliferation.
As with all case reports, limitations of this study include the inability to draw any generalizable conclusions and the inability to establish any cause-and-effect relationship. This study is further limited by its focus on a rare presentation of a common condition in a single patient.
CONCLUSION
This case highlights the unusual presentation of a multiply recurrent calcaneal osteochondroma, emphasizing the need for comprehensive surgical excision and diligent follow-up. The most likely reason for recurrence, as described in the literature, is incomplete resection. While this remains possible, it was considered less likely in this patient, as the initial surgical resection performed by orthopedic oncology (the patient’s third resection) had been intentionally thorough given that the lesion had already recurred twice at that time. It is speculated that mechanical microtrauma to the site may have contributed to recurrence, as the most recent recurrence occurred after a significant increase in walking over several months while the patient was studying abroad. In this patient, the benign nature of the tumor was confirmed through repeated histological analyses and review of prior histological studies. However, whenever a benign tumor recurs, suspicion for malignant transformation should be heightened. Further studies are warranted to better understand the pathogenesis and optimal management of recurrent osteochondromas in atypical locations.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to the paper as follows: D.M.: Contributed to study conception and design; T.S. and D.W.: Carried out data collection; T.S., D.W., and J.K.: Prepared the draft manuscript; J.K.: Contributed to manuscript editing. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| MRI | = Magnetic Resonance Imaging |
| CAM | = Controlled Ankle Motion |
| HMO | = Hereditary Multiple Osteochondromas |
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
CONSENT FOR PUBLICATION
Consent for publication is not applicable to this case report, and all information in this report has been deidentified.
AVAILABILITY OF DATA AND MATERIALS
All data generated or analyzed during this study are included in this published article.
ACKNOWLEDGEMENTS
Declared none.