All published articles of this journal are available on ScienceDirect.

Risk Factors for Early Fracture-related Infection After Surgical Treatment of Ankle Fractures in Patients Aged 50 Years and Older
Authors Info & Affiliations
Abstract
Introduction
Ankle fractures are increasingly common in older adults, with complication rates of up to 30% following surgical treatment. Identifying risk factors for fracture-related infections (FRI) could enable surgeons to reduce the complication rate.
Methods
In this retrospective case-control study, we screened 950 patient records and documented 59 patients aged 50 years and older with an FRI within the first 3 months after operative treatment of an ankle fracture. Cases of FRI were matched with controls without FRI based on age and sex.
Results
The risk factor analyses identified hypoalbuminemia (OR=17,7), non-compliance (OR=5,1), chronic alcohol abuse (OR=5,5), and high-impact trauma (OR=5,1) as patient-related risk factors. Larger blood loss during surgery, malreduction, and difficulties during surgery were identified as modifiable risk factors associated with operative skill level
Discussion
Early FRI occurred in 6.2% of patients, aligning with reported rates in the literature. The study highlights several modifiable factors associated with increased infection risk, including hypoalbuminemia, substance abuse, postoperative non-compliance, and surgical issues such as malreduction and intraoperative difficulties. High-energy trauma was also strongly associated with infection. Open fractures showed a non-significant trend toward higher risk, likely reflecting limited sample size and optimized management protocols. Overall, the findings underscore the importance of addressing patient-related vulnerabilities and ensuring high surgical quality to reduce infection risk in older adults undergoing ankle fracture fixation.
Conclusion
This study highlights the importance of careful patient selection, optimization of modifiable risk factors, and surgical expertise to improve outcomes for patients undergoing ankle fracture fixation.
1. INTRODUCTION
Ankle fractures represent approximately 15% of all operatively treated fractures and show an increasing incidence [1, 2]. The estimated incidence is 184 per 100,000 persons per year [3].
These fractures demonstrate a bimodal distribution, with a peak in younger men and another in older women. Both closed and open fractures in the elderly are most often caused by low-energy trauma, such as simple falls or sports injuries [4, 5]. The frequency of ankle fractures among older adults has risen dramatically, with a reported 315% increase from 1970 to 2000, and further growth is expected in the coming decades [6]. The number is increasing, particularly among older adults, due to several factors. These include an aging population with higher life expectancy, increased prevalence of osteoporosis and other comorbidities that weaken bone quality, as well as greater participation of older individuals in physical activities that expose them to falls and injuries. Additionally, improved diagnostic methods and greater awareness may contribute to more frequent detection and reporting of such fractures [7].
Unfortunately, complication rates after operative treatment of ankle fractures remain high. Reported rates of deep and superficial infections are approximately 7% and 15%, respectively [8, 9].
Recent studies have confirmed that specific comorbidities substantially increase the risk of complications following operative treatment of ankle fractures in older adults. Pilskog et al. identified peripheral arterial disease (OR = 4.2) and congestive heart failure (OR = 4.7) as strong independent predictors of fracture-related infection in a large cohort study [10]. In a nationwide register analysis of more than 83,000 patients, Happonen et al. demonstrated that older adults with diabetes, peripheral vascular disease, and chronic comorbidities such as pulmonary, renal, or hepatic disorders were significantly more likely to develop postoperative complications [11]. Similarly, Han et al. reported that diabetes, obesity (BMI ≥ 28), high-energy injuries, wound contamination, prolonged surgery, and hypoalbuminemia (albumin <35 g/L) were independent risk factors for surgical site infection after open reduction and internal fixation of ankle fractures [12]. Together, these studies underline the consistent impact of both patient-related and injury-related factors on complication risk.
Independent risk factors included tobacco use and surgery duration exceeding 90 minutes (OR 2.0 and 3.7, respectively) [8]. Several other studies reported similar findings, also identifying obesity as an independent risk factor [9, 13].
The complication rate in older adults is significantly higher than in younger patients, with rates reaching up to 25%, and a one-year mortality ranging from 12% to 23% [14, 15]. Age has been shown to be an independent risk factor for adverse events, with an OR of 2.0 [16]. The one-year mortality following ankle fractures in the elderly approaches that of patients with femoral neck fractures and is in contrast to younger patients, in whom complication rates are lower, and mortality is negligible [4].
One study highlights the significance of age 50 as a critical threshold for postoperative complications in patients undergoing ORIF of ankle fractures. Patients over 50 had a higher risk of infection, compared to younger patients [17].
Given the rising incidence of ankle fractures and the high rate of complications, it is important to identify patient-related risk factors for postoperative complications. Some of these factors may be modifiable and thus provide an opportunity to reduce complication rates through targeted interventions.
The aim of this study was to explore potential risk factors for FRI in patients aged 50 years and older undergoing operative treatment of malleolar fractures.
2. METHOD
2.1. Study Design
This was a retrospective case-control study conducted at the Department of Orthopedic Surgery and Traumatology, University Hospital Basel, Switzerland. The study was performed in accordance with the Declaration of Helsinki and was approved by the local ethics committee Northwest and Central Switzerland (Ethikkommission Northwest- und Zentralschweiz, EKNZ 2020_00318). The requirement for informed consent was waived by the ethics committee to be registered in the department's research database.
2.2. Study Population and Endpoints
Patients aged 50 years and older who underwent surgical treatment for an ankle fracture (AO type 44) at our department between 2008 and 2017 and had a minimum follow-up of 3 months were included (Fig. 1). Medical records from 950 patients were screened for FRI, and 59 patients fulfilled the criteria for early FRI within 3 months postoperatively.
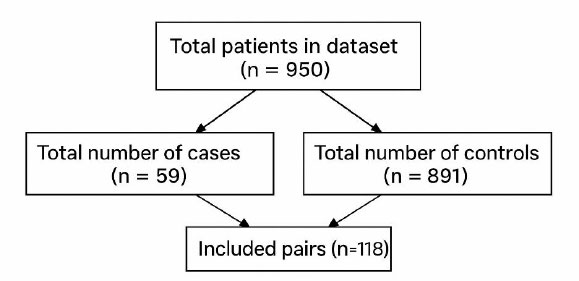
Flowchart of patient selection for the study cohort.
Inclusion criteria:
- Patients aged 50 years or older
- Surgically treated ankle fractures classified as AO/OTA type 44
- Operative treatment performed at the University Hospital Basel between 2008 and 2017
- Minimum postoperative follow-up of 3 months
- Availability of complete electronic medical records, including operative notes and postoperative imaging
- For cases: patients fulfilling the international consensus definition of fracture-related infection (FRI) within 3 months
- For controls: patients without any clinical, radiological, or microbiological signs of infection
Exclusion criteria:
- Patients younger than 50 years
- Non-operatively treated ankle fractures
- Periprosthetic or pathological fractures
- Patients lost to follow-up before 3 months
- Incomplete medical records prevent a reliable assessment of infection status
- Missing or inadequate imaging for postoperative evaluation
2.3. Cases not Meeting the Formal FRI Consensus Definition
FRI was defined according to the international consensus definition [18], requiring at least one of the following five confirmatory criteria:
Fistula, sinus tract, or wound breakdown with communication to bone or implant; Purulent drainage from the wound or visible pus during surgery; Pathogen isolation by culture from at least two separate deep tissue or implant specimens; Presence of microorganisms in histopathological examination using specific staining techniques; Acute inflammatory response with >5 neutrophils per high power field (HPF) in histopathological examination.
Patients with an uneventful postoperative course without signs of infection were considered controls. From a pool of 891 eligible patients, 59 control patients were matched to the FRI cohort based on age and sex.
2.4. Patient Characteristics and Risk Factors
Data for risk factor assessment-including trauma mechanism, fracture characteristics, surgical procedure, relevant comorbidities, and medication use at the time of injury-were retrieved retrospectively from electronic patient records.
In addition to demographic variables, the following risk factors were recorded: body mass index (BMI), American Society of Anesthesiologists (ASA) score, diabetes (uncomplicated or complicated), peripheral neuropathy, neuropsychiatric disorders (e.g., dementia, schizophrenia, depression, psychosis), chronic inflammatory disease, AIDS or HIV, hypoalbuminemia, chronic kidney disease, anemia, Elixhauser comorbidity index, osteoporosis (based on T-score), medication known to impair wound healing, smoking, and chronic alcohol abuse. A full list of variable definitions is provided in Supplementary Material.
Injury-related risk factors included: high- vs. low-energy trauma, open vs. closed fracture, presence of polytrauma, and history of previous surgery at the fracture site.
All fractures were classified according to the AO/OTA classification system based on preoperative radiographs and intraoperative findings. Fractures were grouped as type A, B, or C injuries.
Treatment-related variables included anatomical location of fracture (medial, lateral, posterior), type of implant (plate, screw, or nail), use of a syndesmotic screw, documented intraoperative difficulties, fracture malreduction on postoperative radiographs, surgeon experience level, and postoperative non-compliance.
2.5. Treatment Protocol
All patients with ankle fractures were hospitalized, and surgery was delayed until the swelling had subsided. Postoperatively, mobilization in a cast or boot (Vacuped) with partial weight-bearing for six weeks was prescribed, in addition to pain medication and thrombosis prophylaxis (Rivaroxaban 10 mg daily). Patients treated with a syndesmotic screw were instructed to maintain partial weight-bearing for twelve weeks, with screw removal scheduled in the outpatient clinic at twelve weeks.
2.6. Statistical Methods
Case-control matching was performed using 1:1 propensity score matching with a nearest neighbor algorithm without replacement based on age and sex. A 1:1 matching ratio was chosen for feasibility while maintaining comparability between cases and controls. Matching was limited to these variables because only administrative data were available prior to matching, whereas detailed clinical characteristics required manual archive review of matched patients. Matching was conducted using the R package MatchIt (version 4.5.0).
Descriptive statistics were used to summarize baseline and procedural characteristics. Categorical data were reported as frequencies and percentages; continuous variables were summarized using median and interquartile range (IQR).
Missing data were minimal. One patient had missing body mass index data, and one patient had missing data on postoperative noncompliance. Therefore, analyses were conducted using a complete case approach.
To identify potential risk factors for early FRI, univariable logistic regression analyses were performed. Owing to sparse data and quasi-complete separation in several variables, Firth's bias-reduced logistic regression was used to obtain stable and less biased estimates. Analyses were conducted using the logistf package (version 1.24.1) in R (R Core Team, https://www.R-project .org/). As a sensitivity analysis, conditional logistic regression accounting for the matched pairs was performed for variables without separation, to assess the robustness of the findings to the matched study design. All tests were two-tailed, and a p-value < 0.05 was considered statistically significant.
3. RESULTS
3.1. Baseline Characteristics of the Study Population
During the study period, 950 patients underwent surgical fixation for ankle fractures at our department and met the defined inclusion criteria (Fig. 1). Among them, 59 patients (6.2%) developed a confirmed FRI within 3 months after surgery and were included in the study cohort. All FRI cases required revision surgery. The study cohort was matched to 59 control patients who experienced an uneventful postoperative course. Patient characteristics for both cohorts are summarized in Table 1.
3.2. Risk Factor Analysis
The analysis of risk factors for early postoperative FRI within the first 3 months after ankle fracture fixation is summarized in Table 2. Regarding injury-related variables, patients who sustained high-energy trauma had a fivefold increased risk of developing an infection (OR = 5.1; 95% CI: 1.8-17.4; p = 0.002). Neither polytrauma nor open fractures were associated with a significantly increased risk of infection in this cohort.
|
N (%) - FRI (Study Cohort) |
N (%) - Non-FRI (Control Cohort) |
|
|---|---|---|
| All | 59 (100) | 59 (100) |
| Age (Median & IQR) | 66.1 (56.7 to 76.2) | 66.2 (55.9 to 74.8) |
| Sex | ||
| - female | 40 (67.8) | 46 (78) |
| - male | 19 (32.2) | 13 (22) |
| BMI | 26 (22.8 to 28.4) | 26.1 (24.2 to 29.3) |
| ASA score | ||
| - 1 | 5 (8.5) | 9 (15.3) |
| - 2 | 11 (18.6) | 18 (30.5) |
| - 3 | 40 (67.8) | 24 (40.7) |
| - 4 | 3 (5.1) | 7 (11.9) |
| - 5 | 0 (0) | 1 (1.7) |
| Mechanism of Injury | ||
| - Low impact | 42 (71.2) | 55 (93.2) |
| - High impact | 17 (28.8) | 4 (6.8) |
| Firth's Bias-reduced Logistic Regression | Conditional Logistic Regression | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Coefficients | N - Cases | N - Control | Odds Ratios | CI | P-value | Adjusted P-value* | Odds Ratios | 95%-CI | P-value |
| Sex - Male | 19 / 59 (32.2%) | 13 / 59 (22.03%) | 1.66 | 0.741 - 3.8 | 0.219 | 0.361 | 1.6 | 0.726 - 3.53 | 0.244 |
| Age (increase per year) | 59 | 59 | 1 | 0.976 - 1.03 | 0.858 | 0.914 | 1.04 | 0.934 - 1.15 | 0.506 |
| BMI (increase by one point) | 59 | 59 | 0.988 | 0.924 - 1.05 | 0.715 | 0.842 | 0.986 | 0.92 - 1.06 | 0.695 |
| Diabetes - uncomplicated | 4 / 59 (6.78%) | 2 / 59 (3.39%) | 1.86 | 0.396 - 11.1 | 0.433 | 0.649 | 2 | 0.366 - 10.9 | 0.423 |
| Diabetes - complicated | 4 / 59 (6.78%) | 3 / 59 (5.08%) | 1.31 | 0.305 - 6.09 | 0.714 | 0.842 | 1.33 | 0.298 - 5.96 | 0.706 |
| AIDS or HIV positive | 1 / 59 (1.69%) | 0 / 59 (0%) | 3.05 | 0.159 - 449 | 0.466 | 0.668 | - | - | - |
| Hypalbuminaemia | 38 / 59 (64.41%) | 5 / 59 (8.47%) | 17.7 | 6.82 - 54.4 | <0.001 | <0.001 | 17.5 | 4.21 - 72.8 | <0.001 |
| Bloodloss anemia | 15 / 59 (25.42%) | 0 / 59 (0%) | 41.4 | 5.32 - 5340 | <0.001 | <0.001 | - | - | - |
| Deficiency anemia | 14 / 59 (23.73%) | 5 / 59 (8.47%) | 3.16 | 1.15 - 9.88 | 0.025 | 0.072 | 2.8 | 1.01 - 7.77 | 0.048 |
| Anemia (Combined) | 27 / 59 (45.76%) | 5 / 59 (8.47%) | 8.38 | 3.24 - 25.4 | <0.001 | <0.001 | 6.5 | 2.27 - 18.6 | <0.001 |
| Elixhauser score - increase by one | 59 | 59 | 0.994 | 0.947 - 1.04 | 0.806 | 0.901 | 0.991 | 0.936 - 1.05 | 0.769 |
| Osteoporosis | 9 / 59 (15.25%) | 9 / 59 (15.25%) | 1 | 0.371 - 2.7 | 1 | 1 | 1 | 0.351 - 2.85 | 1 |
| Wound medication | 4 / 59 (6.78%) | 0 / 59 (0%) | 9.65 | 0.995 - 1290 | 0.051 | 0.115 | - | - | - |
| Medication negatively influencing skin healing | 6 / 59 (10.17%) | 1 / 59 (1.69%) | 4.74 | 0.952 - 46.5 | 0.058 | 0.12 | 6 | 0.722 - 49.8 | 0.097 |
| Smoking | 18 / 59 (30.51%) | 10 / 59 (16.95%) | 2.1 | 0.9 - 5.12 | 0.086 | 0.158 | 2.33 | 0.897 - 6.07 | 0.082 |
| High impact fracture | 17 / 59 (28.81%) | 4 / 59 (6.78%) | 5.08 | 1.8 - 17.4 | 0.002 | 0.008 | 7.5 | 1.72 - 32.8 | 0.007 |
| Open fracture | 14 / 59 (23.73%) | 6 / 59 (10.17%) | 2.62 | 0.992 - 7.63 | 0.052 | 0.115 | 3 | 0.968 - 9.3 | 0.057 |
| Renal failure | 10 / 59 (16.95%) | 13 / 59 (22.03%) | 0.731 | 0.291 - 1.79 | 0.493 | 0.678 | 0.625 | 0.204 - 1.91 | 0.41 |
| Syndesmotic screw | 7 / 59 (11.86%) | 14 / 59 (23.73%) | 0.448 | 0.163 - 1.15 | 0.096 | 0.167 | 0.462 | 0.175 - 1.21 | 0.117 |
| Polytrauma | 7 / 59 (11.86%) | 5 / 59 (8.47%) | 1.42 | 0.444 - 4.78 | 0.556 | 0.734 | 2 | 0.366 - 10.9 | 0.423 |
| Difficulties during surgery | 16 / 59 (27.12%) | 5 / 59 (8.47%) | 3.76 | 1.39 - 11.6 | 0.008 | 0.03 | 3.75 | 1.24 - 11.3 | 0.019 |
| Fracture malreduction on postoperative radiographs | 9 / 59 (15.25%) | 0 / 59 (0%) | 22.4 | 2.72 - 2910 | 0.001 | 0.006 | - | - | - |
| Resident/Senior Orthopedic versus Senior Consultant/Head of Dep. | 42 / 59 (71.19%) | 44 / 59 (74.58%) | 0.846 | 0.376 - 1.89 | 0.683 | 0.842 | 0.857 | 0.396 - 1.85 | 0.695 |
| Depression | 10 / 59 (16.95%) | 6 / 59 (10.17%) | 1.75 | 0.62 - 5.26 | 0.293 | 0.461 | 1.67 | 0.606 - 4.59 | 0.323 |
| Neurodegenerative disorders | 11 / 59 (18.64%) | 12 / 59 (20.34%) | 0.901 | 0.364 - 2.21 | 0.819 | 0.901 | 0.889 | 0.343 - 2.3 | 0.808 |
| Psychoses | 18 / 59 (30.51%) | 10 / 59 (16.95%) | 2.1 | 0.9 - 5.12 | 0.086 | 0.158 | 3 | 0.968 - 9.3 | 0.057 |
| Alcohol abuse | 21 / 59 (35.59%) | 5 / 59 (8.47%) | 5.53 | 2.11 - 16.9 | <0.001 | 0.002 | 9 | 2.09 - 38.8 | 0.003 |
| Drug abuse | 9 / 59 (15.25%) | 2 / 59 (3.39%) | 4.33 | 1.16 - 23.4 | 0.028 | 0.072 | 4.5 | 0.972 - 20.8 | 0.054 |
| Post operative non-compliance | 14 / 59 (23.73%) | 3 / 58 (5.17%) | 5.05 | 1.62 - 20.4 | 0.004 | 0.017 | 6 | 1.34 - 26.8 | 0.019 |
| Psychological disorders (Combined) | 36 / 59 (61.02%) | 24 / 59 (40.68%) | 2.25 | 1.09 - 4.72 | 0.028 | 0.072 | 2.33 | 1.07 - 5.09 | 0.033 |
| Psychological disorders or Non-compliance (Combined) | 36 / 59 (61.02%) | 24 / 59 (40.68%) | 2.25 | 1.09 - 4.72 | 0.028 | 0.072 | 2.33 | 1.07 - 5.09 | 0.033 |
Several patient-related factors were significantly associated with higher infection risk. These included hypoalbuminemia, anemia, postoperative non-compliance, and chronic alcohol abuse. Non-compliance and alcohol abuse were both linked to more than a fivefold increased risk of infection. Alcohol abuse was recorded in 21 patients (35.6%) in the FRI group, compared to 5 patients (8.5%) in the control group (OR = 5.5; 95% CI: 2.1-16.9; p < 0.001). Postoperative non-compliance was present in 14 patients (23.7%) in the FRI group and in 3 patients (5.2%) in the control group (OR = 5.1; 95% CI: 1.6-20.4; p = 0.004).
A trend toward increased infection risk was observed in patients with documented drug abuse and psychological disorders, although these associations did not reach statistical significance after adjustment.
Among surgery-related factors, intraoperative difficulties and postoperative fracture malreduction were significantly associated with increased infection risk. Intraoperative difficulties had an OR of 3.8 (95% CI: 1.4–11.6; p = 0.008), while malreduction showed a markedly elevated OR of 23.7 (95% CI: 2.7–291.0; p = 0.001).
4. DISCUSSION
The rate of FRI after ankle fracture surgery was 6.2% in our cohort, which is in line with previously reported rates [8, 9, 13]. This study identified several patient-related factors that substantially increased the risk of postoperative complications. Patients with hypoalbuminemia (OR = 17,7), medication negatively influencing wound healing (OR = 4,7), drug abuse (OR = 4,3), high-energy trauma (OR = 5,1), and open fractures (OR = 2,6) were at particularly high risk for infection. Recent multicenter data confirm that high-energy mechanisms substantially increase postoperative complication rates after ankle fracture fixation. These risk factors are not specific to elderly patients and are consistent with findings from earlier studies [8, 9, 19,]. These findings provide a basis for hypothesis generation and future prospective validation.
However, in contrast to younger individuals, the importance of achieving anatomic reduction may be less critical in older patients. The use of intramedullary fibula nails, for example, often results in a non-anatomic reduction, yet has shown good functional outcomes and lower rates of wound complications [20]. Similarly, surgical treatment of the medial malleolus can be modified. In older patients with bimalleolar fractures, functional outcomes after fixation of only the lateral malleolus were comparable to those in patients with full bimalleolar fixation [21]. Therefore, in older patients with one or more of the risk factors described above, surgeons may consider less invasive techniques to reduce the complication rate. Contemporary population-based studies likewise report elevated complication and mortality rates in older adults sustaining ankle fractures.
Certain surgical factors were also associated with increased risk of infection. These included malreduction (OR = 22,4) and technical difficulties during surgery (OR = 3,8). All of these are modifiable and likely related to the surgeon's level of experience. The variable "odifficulties during surgery" captured intraoperative challenges such as prolonged operative time due to poor visualization, difficulties with soft tissue handling, the need for unplanned additional fixation, or challenges related to fracture complexity. This category is broad and subjective and lacks granularity, but emphasizes that ankle fracture surgery is unforgiving and should be conducted by experienced surgeons.
In a study of 478 patients with ankle fractures treated by a single experienced surgeon, the revision rate was only 1%, and the infection rate was below 3%-substantially lower than in most published series, including the present study [19]. This suggests that surgical skill and experience play a key role in outcomes. Although ankle fractures are often used as training cases for junior surgeons due to the standardized technique and straightforward anatomy, this approach should be reconsidered in light of the relatively high complication rates reported in the literature. In our cohort, we found no significant difference in infection rates between patients treated by junior versus senior surgeons, probably because junior surgeons always operate on ankle fractures supervised by senior surgeons in our institution
Interestingly, patients with a syndesmotic screw had fewer infections than patients without a syndesmotic screw. Since all fractures in this study were classified according to the AO/OTA system, this finding can be interpreted in the context of injury severity and fracture morphology. Syndesmotic fixation is typically required in AO type C fractures, which are located more proximally and are often amenable to closed reduction or minimally invasive fixation. These techniques are associated with less soft tissue trauma and potentially lower infection risk. Furthermore, the proximal location of the fracture offers better soft tissue coverage compared to distal fibular fractures, which are more vulnerable to wound healing complications. The presence of the screw also enhances mechanical stability, potentially limiting micromotion and supporting tissue healing. Taken together, these factors may explain the lower FRI rate observed in patients who received syndesmotic screws.
Polytrauma was more frequent in the infection group of our cohort (11.9% vs. 8.5%), with an odds ratio of 1.4 (95% CI 0.4-4.7), but the association was not statistically significant (p = 0.556). This aligns with current evidence, as no recent studies have identified polytrauma as an independent risk factor for infection specifically in operatively treated ankle fractures. A likely explanation is that polytrauma patients are predominantly treated in specialized trauma centers, where strict management protocols and multidisciplinary care may reduce the expected infection risk [22]. Findings from larger trauma datasets also show inconsistent associations between polytrauma and postoperative infection, supporting the limited independent effect observed in our cohort.
Open fractures, in contrast, demonstrated a stronger trend in our data: they were present in 23.7% of the infection group compared with 10.2% of controls, corresponding to an odds ratio of 2.6 (95% CI 1-7.6). While this association approached significance (p = 0.052), it ultimately did not reach the conventional threshold. Nevertheless, this finding is consistent with recent large studies. A Dutch multicenter cohort of 929 surgically treated ankle fractures reported open fracture as an independent predictor of SSI (p = 0.004; deep SSI p = 0.002), and a national cohort of more than 40,000 patients likewise identified open fractures as one of the strongest risk factors (OR = 4.2; p < 0.001). The lack of statistical significance in our study may reflect limited sample size as well as optimized management strategies, including early debridement, antibiotic prophylaxis, and staged reconstruction, which can mitigate the classical infection risk [23, 24].
Although diabetes is a well-established risk factor for FRI in the literature, it was not found to be a significant predictor in our cohort. This may be due to several factors. First, diabetic patients in our study might have had relatively well-controlled disease, as many were under regular medical supervision and received perioperative glucose management. Second, our definition of diabetes did not include measures of glycemic control, such as HbA1c levels, which may better reflect the patient's immunological and microvascular status. Third, the relatively small number of diabetic patients may have limited the statistical power to detect a significant association. Future studies incorporating glycemic control parameters and larger sample sizes may better elucidate the true impact of diabetes on FRI risk.
We also found that psychological disorders significantly increased the risk of infection (OR = 2.3), with dementia and depression being the most commonly documented diagnoses. Although rarely discussed in trauma literature, this finding is supported by data from chronic wound studies. In one study of 53 elderly patients with lower leg ulcers, individuals with high levels of depression and anxiety (measured by the Hospital Anxiety and Depression Scale) were four times more likely to experience delayed healing. Several other observational and experimental studies have shown that stress and anxiety impair wound healing, especially in older adults [25, 26]. Interventions aimed at stress modulation have been shown to improve healing outcomes in this population [27]. It is therefore plausible that addressing psychological stress in patients with ankle fractures may reduce the risk of postoperative complications.
Fracture-related infection in older adults should be viewed as the result of a multifactorial interaction between systemic vulnerability, impaired bone and soft-tissue biology, and surgical stress. Age-related alterations in nutritional status, inflammatory response, and tissue regeneration capacity may collectively reduce host resilience and contribute to increased infection susceptibility.
Given the retrospective design and limited sample size, the observed associations should be interpreted cautiously and primarily regarded as hypothesis-generating. Our findings contribute to an evolving evidence base and aim to support clinical risk awareness rather than establish causal relationships.
5. LIMITATIONS
This study has several limitations that should be considered when interpreting the findings. First, the retrospective design inherently carries risks of selection bias and incomplete documentation, as data extraction relied on existing medical records. Second, the relatively small number of FRI cases limited the statistical power, especially for less frequent risk factors such as polytrauma or open fractures, which may explain why some clinically relevant trends did not reach statistical significance. Third, matching was restricted to age and sex, and a 1:1 matching ratio was used for feasibility, as detailed clinical characteristics and comorbidities were only available after manual archive review. Consequently, residual confounding cannot be excluded, and only univariable analyses were performed. Fourth, the study was conducted in a single tertiary center with established treatment protocols, which may restrict the generalizability of the results to other healthcare settings. Finally, factors such as glycemic control, nutritional status over time, or detailed psychosocial variables were not available for all patients and could not be included, highlighting the need for prospective multicenter studies to further validate these findings. Accordingly, the findings provide hypotheses for future prospective and multicenter investigations.
CONCLUSION
Patients with high-energy ankle fractures and open fractures showed an increased risk of early postoperative fracture-related infection. In addition, hypoalbuminemia, anemia, drug abuse, psychological disorders, and medications known to impair wound healing were associated with higher infection rates. Surgery-related factors such as fracture malreduction and technical difficulties during the procedure were also linked to increased complication risk.
These findings highlight that operative treatment of ankle fractures in patients aged 50 years and older is associated with substantial risk. Given the retrospective and exploratory nature of this study, the observed associations should be interpreted cautiously and do not imply causality. Nevertheless, identification of high-risk patients and attention to potentially modifiable surgical factors may contribute to improved perioperative management and risk awareness. Further prospective studies are required to validate these findings.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: M.N.: Study conception and design, data collection, analysis and interpretation of results, manuscript drafting; M.M.: Study conception and design, supervision; F.S.H.: Statistical analysis and interpretation of data; H.E.: Study supervision and critical revision. All authors reviewed and approved the final manuscript.
LIST OF ABBREVIATIONS
| FRI | = Fracture-related infection |
| ASA | = American Society of Anesthesiologists |
| BMI | = Body mass index |
| OR | = Odds ratio |
| CI | = Confidence interval |
| SSI | = Surgical site infection |
| AO/OTA | = Arbeitsgemeinschaft fA1/4r Osteosynthesefragen / Orthopaedic Trauma Association |
| HPF | = High power field |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was obtained from the Ethics Committee of Northwest and Central Switzerland (EKNZ), reference number: 2020-00318.
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT TO PARTICIPATE
All participants provided written general consent for the use of anonymized data for research purposes.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of this study are available from the corresponding author [M.N] upon reasonable request due to institutional and ethical restrictions. The data are not publicly available as they contain information that could compromise patient privacy.
ACKNOWLEDGEMENTS
Declared none.