All published articles of this journal are available on ScienceDirect.

Total Knee Arthroplasty in Lubumbashi (DR Congo): Preliminary Results in a Low-Resource Setting
Authors Info & Affiliations
Abstract
Introduction
Total Knee Arthroplasty (TKA) is the gold standard treatment for advanced gonarthrosis, but its availability remains limited in low-resource settings. This study presents preliminary outcomes of TKA performed in Lubumbashi.
Methods
A retrospective, single-center study was conducted on patients who underwent TKA between August 2017 and August 2024. Data collected included demographic, clinical, radiological, and functional variables. Pre and postoperative assessments were based on the International Knee Society (IKS) score. All surgeries were performed using posterior-stabilized prostheses. Postoperative follow-up averaged 24 months.
Results
A total of 27 patients were included in this series. The mean age was 63.3 years, with a female predominance (sex ratio 0,7). Gonarthrosis was primary in 82% of cases, with advanced radiographic stages Ahlbäck IV-V in 89%. The average preoperative IKS score was 104, improving to 172 postoperatively. Complications included one hematoma, one deep vein thrombosis, two superficial infections, and two cases of late-onset medial laxity. Two patients experienced persistent severe pain, and two cases of prosthetic loosening were detected after two years. Overall, 82.5% of patients achieved good to excellent outcomes.
Discussion
This study confirms that total knee arthroplasty is feasible and effective in a resource-limited environment when surgical technique and perioperative management are adapted to local constraints. Despite infrastructural and economic barriers, functional outcomes and complication rates were comparable to other African series. The progressive improvement observed reflects the institutional learning curve, strengthened by international collaboration and protocol standardization. Persistent challenges include limited implant supply, inadequate rehabilitation infrastructure, and lack of health insurance coverage. Expanding training programs, improving logistics, and developing regional arthroplasty registries remain essential for sustainable progress.
Conclusion
TKA can be successfully implemented in sub-Saharan provided that surgical indications are appropriate and perioperative protocols are rigorously applied
1. INTRODUCTION
Knee osteoarthritis is a prevalent degenerative joint disease and one of the leading causes of pain-related disability in older adults worldwide [1]. It results from a progressive breakdown of articular cartilage, often accompanied by subchondral bone remodeling, which ultimately leads to chronic pain, joint stiffness, and progressive loss of mobility.
In the Democratic Republic of the Congo, particularly in the Haut-Katanga region, knee osteoarthritis is being diagnosed with increasing frequency. This rise is closely linked to demographic ageing, rapid urbanization, and the growing exposure to risk factors such as obesity and inadequately managed joint trauma [2, 3]. Despite this increasing burden, access to definitive surgical treatment remains limited.
Total Knee Arthroplasty (TKA) is widely recognized as the reference treatment for advanced and disabling gonarthrosis, offering durable pain relief and marked functional improvement when conservative measures fail [4]. However, in low-resource settings, access to TKA remains severely constrained by high costs, scarcity of trained arthroplasty surgeons, limited rehabilitation services, and insufficient health infrastructure [5, 6].
In Lubumbashi, Medpark Clinic performed its first TKA on August 19, 2017, becoming the only facility in the region to provide this procedure on a regular basis. This initiative was developed despite important technical and human-resource limitations. Although the demand for TKA continues to grow, mainly among patients with advanced primary osteoarthritis, the number of procedures performed remains modest.
Multiple barriers continue to restrict the expansion of arthroplasty services, including the high cost of implants, limited access to specialized training, suboptimal postoperative rehabilitation, and the absence of universal health insurance coverage. In addition, incomplete surgical infrastructure complicates the management of intraoperative difficulties and postoperative complications, both of which are critical for the long-term safety of joint replacement programs [7].
Within this context, the present study aims to report the clinical and functional outcomes of a series of TKA procedures performed at Medpark Clinic between 2017 and 2024, with particular attention to patient characteristics, surgical practices, postoperative evolution, and medium-term results.
2. METHODS
2.1. Study Design
This was a monocentric, retrospective, continuous observational case series conducted at Medpark Clinic in Lubumbashi, in the southeastern region of the Democratic Republic of the Congo, a level 4 referral hospital affiliated with the University of Lubumbashi. Established in 2016, the clinic serves as a national reference center and collaborates with specialists from South Africa. The first total knee arthroplasty was performed in February 2017, positioning the institution as a pioneer in knee arthroplasty in the region.
2.2. Population and Data Collection
Eligible participants included those who received a primary TKA and had a functional follow-up of at least 12 months, while patients lost to follow-up before 12 months or those who underwent revision arthroplasty were excluded. Data were collected using a standardized extraction form and comprised demographic characteristics, clinical status, radiographic assessments, and surgical details. Postoperative information included complications, radiological outcomes, functional recovery, and overall patient satisfaction.
2.3. Functional Evaluation
The functional outcomes were assessed using the IKS score [8], which includes two components: the clinical score (pain, stability, range of motion) and the functional score (walking ability, stair climbing, and use of walking aids). Scores were recorded preoperatively and at the latest follow-up (12 months or more after surgery). Results were categorized as follows: Excellent: > 80 points, Good: 70 -79 points, Fair: 60 - 69 points, Poor: < 60 points.
2.4. Radiological Evaluation
The preoperative radiological assessment was based on standard weight-bearing anteroposterior and lateral radiographs of both knees, allowing precise analysis of the joint space, subchondral bone density, and the presence of osteophytes or geodes. Radiological findings were graded according to the Ahlbäck classification [9]. The posteroanterior 45° flexion view (Schuss view) provided better visualization of the posterior femoral condyles and deep cartilage lesions, particularly in the medial femorotibial compartment. A full-length standing radiograph (pangonogram) of the lower limb, extending from the hip to the ankle, was also performed. This examination aimed to measure the Hip-Knee-Ankle (HKA) angle (< 180° = genu varum, > 180° = genu valgum),
The postoperative radiological evaluation assessed the quality of prosthetic fixation and implant positioning by measuring the α (alpha), β (beta), γ (gamma), and δ (delta) angles, as well as the patellar height according to the Caton-Deschamps index.
At long-term follow-up, radiographs were reviewed for signs of polyethylene wear, aseptic loosening, or osteolysis, based on the Ewald radiographic criteria [10].
2.5. Statistical Analysis
Data were entered and coded using Microsoft Excel 2013 and analyzed with Epi Info (version 7.1.0.6). Descriptive statistics were used to summarize the study population and outcomes. Quantitative variables were expressed as mean ± standard deviation, and qualitative variables were reported as absolute frequencies and relative percentages. Results were presented in tables and figures to enhance clarity and facilitate interpretation.
2.6. Ethical Considerations
The study protocol was reviewed and approved by the Ethics Committee of the University of Lubumbashi (Reference: UNILU/CEM/131/2022). Given the retrospective design, informed consent was waived, and all data were handled in strict compliance with confidentiality and patient anonymity requirements.
3. RESULTS
3.1. Epidemiological and Clinical Characteristics
A total of 27 patients, representing 29 total knee arthroplasties, were included in the study. The mean age of the cohort was 63.3 years (Fig. 1), and a female predominance was observed (n=20, 74%, sex ratio (M/F) of 0.7). Relevant medical histories included two cases of previous tibial fractures, two patients with prior total hip arthroplasties, and four patients with inflammatory conditions (three with rheumatoid arthritis and one with ankylosing spondylitis). Obesity was documented in four cases, all of whom were female, with a mean body mass index (BMI) of 31.6. The right knee was more frequently involved, accounting for 69% of procedures (n= 20). Only one patient underwent bilateral TKA. Primary osteoarthritis was the leading surgical indication, observed in 82% of cases (Table 1). All patients reported mechanical knee pain; 26% had an additional inflammatory component. More than 80% experienced painful and limited range of motion, and 69.5% exhibited an antalgic gait. The interval between the onset of initial joint pain and the first specialized consultation for arthroplasty varied considerably, ranging from 2 to 18 years. The most frequent axial deformity was genu varum (60.8%). The mean preoperative knee flexion was 105°, and the mean preoperative IKS score was 104 out of 200.
| Type of Indication | Number of Cases | Percentage (%) |
|---|---|---|
| Primary osteoarthritis (gonarthrosis) | 23 | 85.1 |
| Post-traumatic secondary osteoarthritis | 2 | 7.4 |
| Rheumatoid arthritis-related gonarthrosis | 1 | 3.7 |
| Ankylosing spondylitis-related gonarthrosis | 1 | 3.7 |
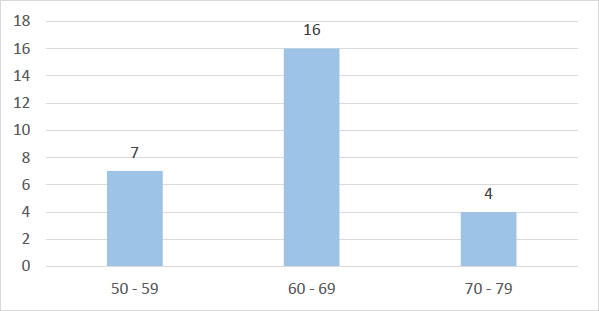
Age distribution of patients undergoing total knee arthroplasty.
3.2. Radiological Assessment
All patients exhibited advanced disease corresponding to stages IV or V (Fig. 2a,b). The full-length standing radiograph was performed in only three patients. The mean HKA angle was 171.35° ± 10°, indicating a mild global varus alignment of the mechanical axis of the lower limb.
3.3. Operative Data
All patients were positioned in the supine position (Fig. 3a), and general anaesthesia was administered in 81.4% (n= 22) of cases. A standard medial parapatellar approach was used for all procedures (Fig. 3b). The operative sequence (Fig 4a-d) varied according to the surgeon’s preference. In the majority of cases (n = 24; 82.8%), surgery began with the proximal tibial cut, while in five cases (17.2%), it started with the distal femoral cut. All arthroplasties were performed using Posterior-Stabilized (PS) prostheses, without preservation of the anterior or posterior cruciate ligaments. Each knee underwent osteophyte excision and circumferential patellar denervation using electrocautery, except in two cases where patellar resurfacing was performed because of severe femoropatellar degeneration or advanced chondropathy. All prostheses were cemented, both on the femoral and tibial sides. The mean operative time was approximately 120 minutes.
3.4. Postoperative Management
All patients received perioperative antibiotic prophylaxis with Ceftriaxone (1 g every 8 hours for 48 hours) and Gentamicin (40 mg/day for 3 days); Amoxicillin-clavulanic acid was used in cases of β-lactam allergy. Non-Steroidal Anti-Inflammatory Drug (NSAIDs) were routinely prescribed for 5-7 days, except in patients with contraindications, and combined with Omeprazole (20 mg/day) for gastric protection.
Postoperative analgesia followed a two-phase protocol, such as (1) intravenous Paracetamol + Tramadol during the first 48 hours, supplemented by NSAIDs when tolerated, and (2) oral analgesics adjusted to the Visual Analogue Scale (VAS) thereafter. Morphine was reserved for refractory or severe acute pain. Thromboprophylaxis with low-molecular-weight heparin (Enoxaparin 40 mg/day subcutaneously) was initiated within hours after surgery and continued for 21 days. High-risk patients underwent biological monitoring of platelet count and serum creatinine.

Bilateral anteroposterior ( a ) and lateral ( b ) weight-bearing radiographs of the knees showing bilateral medial compartment osteoarthritis, more pronounced in the left knee associated with varus deformity, stage IV and V according to Ahlbäck.
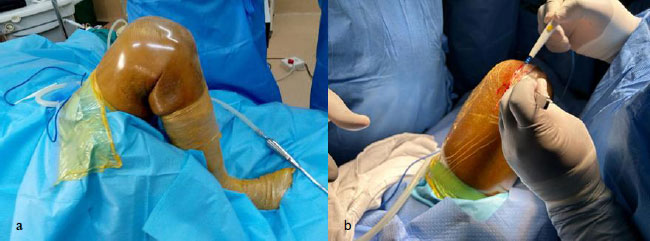
(a) Patient positioning on the operating table in the supine position with two lateral supports; (b) medial parapatellar skin incision.
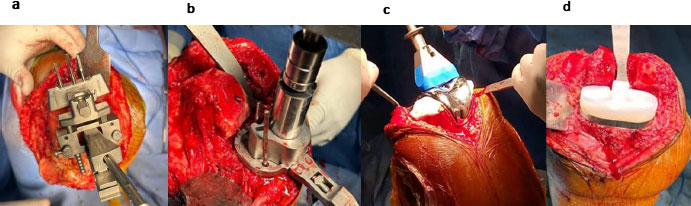
Total knee prosthesis components and surgical steps: (a) distal femoral cut; (b) preparation for tibial implant; (c) definitive femoral component; (d) polyethylene insert.
Rehabilitation started on postoperative day one, aiming for early mobilization, thromboembolic prevention, and functional recovery. Exercises progressed from active–passive mobilization (0-45°) and quadriceps strengthening to assisted ambulation, with gradual flexion up to 100 -120°. By the final follow-up, all patients achieved independent gait and received advice on weight control and infection prevention.
3.5. Complications and Outcomes
The average hospital stay was 10 ± 6 days (range: 5-30), and no major intraoperative complications were reported. In the early postoperative period (within 30 days), one case of postoperative hematoma occurred without functional impairment or need for surgical revision. One patient developed a Deep Vein Thrombosis (DVT) on the sixth postoperative day, successfully treated with Low-Molecular-Weight Heparin (LMWH) followed by an oral anticoagulant, with no pulmonary embolism. Additionally, two cases of superficial wound infection required surgical irrigation under anesthesia, with microbiological sampling and targeted antibiotic therapy, without progression to deep infection. During the late postoperative period (beyond one month) and over a mean follow-up of 24 months, one patient experienced chronic residual knee pain without instability or radiological loosening, while another developed postoperative stiffness (flexion limited to 50°) in the context of progressive rheumatoid arthritis despite active rehabilitation.
3.6. Functional Evaluation
Postoperative pain was evaluated using the Visual Analogue Scale (VAS), ranging from 0 (no pain) to 10 (worst imaginable pain). At the final follow-up, 18 patients (66.6%) reported no pain (VAS = 0), six patients (22.2%) experienced mild or occasional pain (VAS ≤ 3) compatible with normal daily activities, two patients (7.4%) reported moderate occasional pain (VAS 4-6) without significant functional limitation, and one patient (3.7%) presented with persistent moderate pain (VAS = 6) requiring prolonged analgesic therapy. No patient reported severe pain (VAS ≥ 7). All patients achieved a knee flexion greater than 110°, and no case of severe motion limitation was observed. Overall, the mean flexion range improved from 105.4° ± 24° preoperatively to 130.0° ± 25.5° at the final follow-up, indicating a marked functional gain. In addition, 24 patients (88.9%) demonstrated a significant improvement in walking distance, achieving autonomous ambulation with or without walking aids at a minimum follow-up of six months.
3.7. Radiological Evaluation
Standard anteroposterior and lateral radiographs were used to verify the proper positioning of femoral and tibial components (Fig. 5). However, a postoperative pangonogram, which would have allowed precise measurement of the mechanical axis (HKA), was not routinely performed due to its limited availability and high cost in our setting. This represents a limitation in the accurate evaluation of axial corrections in this study.
Regarding implant positioning, in our series:
- 21 knees (72.4%) showed a femoral component perpendicular to the mechanical axis with a mean α angle of 90° ± 4°; (Fig. 6)
- 18 knees (62.1%) had a tibial component perpendicular to the mechanical axis (β angle = 89° ± 8°);
- On the sagittal plane, 17 knees (58.6%) presented a well-aligned femoral component (γ angle = 0° ± 2°) and 16 knees (55.2%) a physiological tibial slope (δ angle = 0° ± 2°).
- The patella was centered in all knees, reflecting good patellar tracking and balance.
A femoral notch (anterior cortical cut) was observed in three cases, without notable clinical consequences. Two cases of prosthetic loosening were detected after two years postoperatively, occurring in one obese patient (Fig. 7a,b) and in one patient with rheumatoid arthritis.

Postoperative anteroposterior and lateral radiographs showing proper positioning of the prosthesis in a patient operated on for primary knee osteoarthritis.

Postoperative radiograph showing a right total knee arthroplasty with the femoral component positioned perpendicular to the mechanical axis, corresponding to a mean α angle of 90° ± 4°.
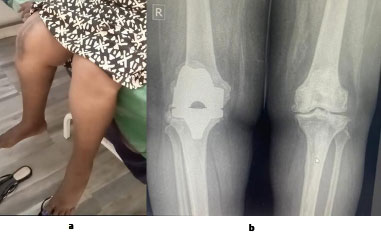
(a) A 56-year-old obese female patient (BMI = 42): (b) radiograph of both knees showing early loosening of the tibial baseplate and marked polyethylene insert wear at two-year follow-up of a right total knee arthroplasty; severe left knee osteoarthritis, classified as Ahlbäck stage IV.

A 67-year-old patient at postoperative day 28 following right total knee arthroplasty. The patient demonstrates knee flexion greater than 110 degrees, full extension, and satisfactory correction of the right lower limb axis.
3.8. Overall Functional Outcomes
The mean IKS score improved from 104 preoperatively to 172 postoperatively, indicating substantial functional recovery (Fig. 8). At final follow-up, the overall functional outcomes were distributed as follows: Excellent in 60.8% of cases, Good in 21.7%, Fair in 13%, and Poor in 4.3%.
4. DISCUSSION
This study provides original, context-specific data on the early outcomes of total knee arthroplasty in the southeastern Democratic Republic of the Congo. In this region, locally generated evidence on joint replacement surgery remains scarce. Our results demonstrate that, even in a resource-limited environment, TKA can lead to clinically meaningful improvements in pain relief, functional capacity, and gait autonomy, while maintaining an acceptable complication rate.
These findings directly address the main objectives of our study. Firstly, they confirm that TKA is technically feasible and clinically effective in our setting. Secondly, they show that substantial functional recovery can be achieved despite delayed presentation and advanced disease stages. Thirdly, although complication rates are higher than those reported in high-income countries, they remain comparable to those observed in other African series.
4.1. Late Presentation and Preoperative Characteristics
A notable feature of our cohort is the prolonged delay, often spanning several years, between symptom onset and the first orthopedic consultation. This delay largely explains the predominance of advanced radiographic stages and the high frequency of varus deformities at presentation. Similar patterns have been consistently reported across sub-Saharan Africa [11-16] and reflect structural barriers such as limited financial access to care, lack of health insurance, and insufficient awareness of early osteoarthritis management.
The female predominance and the high proportion of primary osteoarthritis observed in our series are consistent with demographic trends reported in both African and Western populations. Although obesity and inflammatory arthritis were present, they did not represent the dominant etiological factors in our cohort.
4.2. Surgical Feasibility and Technical Considerations
Despite significant resource constraints, all procedures were performed using a standardized and reproducible surgical technique. The medial parapatellar approach, employed in all cases, remains a reliable and versatile exposure for primary TKA and is widely used in African arthroplasty series [14, 15].
An important determinant of feasibility in our context was the development of a structured partnership with South African arthroplasty teams, combined with improved access to a reliable implant supply chain. Prior to this collaboration, many Congolese patients were compelled to seek surgical care abroad, particularly in India, South Africa, or Europe. The establishment of local implant availability and surgeon training has significantly strengthened local capacity and contributed to the sustainability of arthroplasty services.
4.3. Functional Outcomes
Patients in our series experienced marked reductions in pain and meaningful gains in mobility, as demonstrated by improved IKS scores and the high proportion of patients achieving independent ambulation. These results are in line with other African reports [13, 14] and confirm that modern arthroplasty techniques can yield satisfactory functional outcomes even in constrained environments.
When compared with European and North American series, where functional success rates frequently exceed 90% [17-22], our outcomes remain within an acceptable range. The slightly lower performance observed is likely related to contextual factors, including delayed surgical indication, more severe preoperative deformities, and limited access to structured physiotherapy.
4.4. Complications
The overall complication rate of 20% observed in our study is comparable to rates reported in other African cohorts [11, 13-16], although higher than the 5-8% typically described in high-income settings. This difference likely reflects the early developmental phase of the arthroplasty program, heterogeneity in postoperative rehabilitation, and the presence of comorbidities such as obesity and inflammatory arthritis.
Importantly, no deep infections were recorded, and all early complications were managed successfully using standardized perioperative protocols and infection-prevention measures in line with international recommendations [23-26]. The two cases of aseptic loosening occurred in patients with recognized risk factors, namely obesity and rheumatoid arthritis, supporting existing evidence regarding their contribution to mechanical failure.
4.5. Radiological Alignment
Although postoperative alignment assessment was limited by the absence of routine long-leg radiographs, most components were positioned within acceptable angular ranges. This suggests satisfactory technical execution despite restricted access to advanced imaging. Nevertheless, the lack of systematic hip–knee–ankle measurements remains a limitation for precise evaluation of mechanical axis restoration.
4.6. Strengths and Limitations
This study has several limitations, including its retrospective design, small sample size, and single-center setting, which may limit external validity. The absence of systematic long-leg radiographs further restricts detailed radiological analysis.
However, the study also presents notable strengths: a homogeneous patient cohort, standardized indications, procedures performed by a single surgeon using a consistent technique, a uniform rehabilitation protocol, and independent clinical and radiological assessments. Together, these factors enhance the internal consistency and reliability of the reported outcomes.
CONCLUSION
Our experience demonstrates that effective and safe total knee arthroplasty programs can be implemented in resource-limited settings through targeted international partnerships, investment in surgical training, and standardized care pathways. Expanding access to physiotherapy, reducing financial barriers, and improving public awareness may further optimize outcomes. Future multicenter studies with larger cohorts and longer follow-up are needed to better characterize implant survival and identify predictors of functional recovery in African contexts.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: C.S.M.: Study conception and design; Y.Y., D.M., Y.K.: Data collection; S.D., M.K., D.M., E.S.: Analysis and interpretation of results; C.T., A.M.: Draft manuscript preparation. All authors reviewed the results, contributed to the discussion, and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| BMI | = Body Mass Index |
| CEM | = Medical Ethics Committee |
| DRC | = Democratic Republic of the Congo |
| DVT | = Deep Vein Thrombosis |
| IKS | = International Knee Society |
| LMWH | = Low-Molecular-Weight Heparin |
| NSAID | = Non-Steroidal Anti-Inflammatory Drug |
| PS | = Posterior-Stabilized |
| TKA | = Total Knee Arthroplasty |
| UNILU | = University of Lubumbashi |
| VAS | = Visual Analogue Scale |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was obtained from the Ethics Committee of the University of Lubumbashi (UNILU/CEM/131/2022).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
All data generated or analyzed during this study are included in this published article.
ACKNOWLEDGEMENTS
We sincerely thank Dr. Saleh A (South Africa) for introducing advanced hip and knee arthroplasty techniques in Lubumbashi. His strong skills and dedication have greatly helped our team and improved the quality of care for patients in our region.
We also warmly thank Dr. Kumasamba (South Africa) for his mentorship and hands-on training. His support has strengthened our orthopedic practice and contributed to better surgical results and improved patient quality of life.